The Epiphany Club
Research and clinical physiotherapists in Yorkshire have started meeting on a regular basis for mutual support, to share ideas and to improve their capacity for communication and working together. This is the Epiphany Club, an informal group of physios and other AHPs gathering every few months in a pub near to Leeds Town Centre.
Click to enlarge
Critically Appraised Topics
One well-received proposal for the Epiphany Club was the development of Critically Appraised Topics (CAT). Keele University School of Health and Rehabilitation has produced a number of very useful musculoskeletal CATs and, over the last fifteen years, their collaboration with clinicians has developed into a hugely beneficial, productive and closely-knit team. A CAT is:"a summary of the best available evidence, which answers a clinical question and includes a clinical ‘bottom-line’. A CAT is essentially patient-based, in that it begins with a clinical question generated from a specific patient situation or problem."
This blog will describe the development of the first CAT and its clinical bottom line, generated from the best available evidence.
Background
No sooner had the CAT idea been put forward than a clinical problem cropped up that was ideal for a CAT. The problem had arisen in a ward-based neuro rehabilitation setting and was causing some anxiety among members of the neuro rehab team.After mobilising a patient with an acute partial spinal cord injury, a registrar who had worked at a specialist spinal centre suggested that mobilising patients was inappropriate. He described the current protocol at specialist centres as six weeks' 'bed rest' (or 'Active Bed Based Rehabilitation'). In contrast, the standard procedure on the Leeds Trust rehabilitation unit was early mobilisation when safe to do so (i.e. when medically and surgically stable). But what evidence was there for or against either approach? This then was a clinical question generated by a problem with a specific patient situation, and ideal for a CAT.
Further information: Sir Ludwig Guttmann
There is no doubt that Sir Ludwig Guttmann was a remarkable physican and inspirational human who transformed the quality of care, quality of life and extended the lives of people with spinal cord injuries. The prevailing thought pre-1945 was that rehabilitation was "irrational" and death was inevitable within months, but the principles that he laid down in 1945 were responsible for transforming the outlook and prognosis of people with spinal cord injury. These principles included, for example, the routine turning of patients to prevent skin breakdown. They have remained apparently unchallenged as core practice until at least 1979, but while nobody suggests that turning bedbound patients is not best practice, what is the case for bed rest or against mobilising?
Clinically Appraised Topic (CAT): mobilising acute partial Spinal Cord Injury patients
This Clinically Appraised Topic (Foster et al., 2001) was conducted by Leeds Teaching Hospitals NHS Trust Neurological Rehabilitation team, the Academic Department of Rehabilitation Medicine (University of Leeds) and Leeds Teaching Hospitals Library & Evidence Research Centre, It is described using the the format of the Keele University CATs.
Acknowledgements
The CAT team would like to thank Kay Stevenson (Consultant Physiotherapist and Clinical Champion, Honorary Lecturer, School of Health and Rehabilitation, Keele University) for her guidance and support leading up to and during the development of this Clinically Appraised Topic.

Specific question
(click to enlarge)
Clinical bottom line
There was no evidence against mobilising people with partial spinal cord injury (SCI) who are medically and surgically stable less than six weeks after injury. There were no adverse events reported in stable patients with SCI who received early mobilisation.
There was no evidence that bed-based rehabilitation improves outcomes in comparison to early mobilisation in stable patients with partial SCI.
Why is this important?
Once medically and surgically stable, people with acute partial SCI are managed differently in the first six weeks of their rehabilitation depending on the opinion of the professionals caring for them as to best practice. Some centres favour early mobilisation and others support a period (at least six weeks) of active bed-based rehabilitation.
Inclusion criteria
Patients with acute partial Spinal Cord Injury.
Search strategy
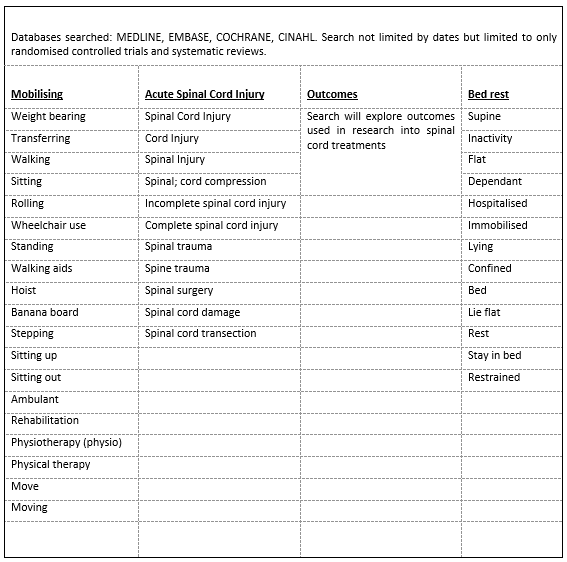
Search terms and databases
(click to enlarge)
Papers found and selection filter

Flow chart
(click to enlarge)
Summary and assessment of quality of papers
Quality of papers assessed using CASP Systematic review checklist(Critical Appraisal Skills Programme, 2018b) and RCT checklist(Critical Appraisal Skills Programme, 2018a) |
| Click to enlarge |
 |
| Click to enlarge |



{kind=link}
Summary
There is no evidence that early mobilisation is harmful for
acute SCI patients who are medically and surgically stable. Studies are of generally
poor quality and do not directly answer the CAT question.
Evidence from one high quality RCT suggests that overground
mobility training is better than body-weight supported treadmill training in
acute (2 – 26 weeks) partial SCI patients. There was a positive effect of early
exercise on muscle tissue within the first 3–6 months post SCI but these were
poor quality studies.
There were weak recommendations in one poor quality paper
for early rehabilitation in patients with traumatic SCI when they are medically
stable and can tolerate treatment.
There is no evidence supporting six weeks of bed rest.
Suggestions for research
This CAT suggests that properly-conducted research is needed to investigate which approach has better outcomes for people with acute partial spinal cord injury. Given numbers of injuries, this would need to be a large multicentre trial exploring multiple outcomes and long term follow ups.References
BAGNALL, A. M.,
JONES, L., DUFFY, S. & RIEMSMA, R. P. 2008. Spinal fixation surgery foracute traumatic spinal cord injury. Cochrane
Database Syst Rev, Cd004725.
CRITICAL APPRAISAL SKILLS PROGRAMME. 2018a. CASP Randomised Control Trial Checklist [Online]. Available: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Systematic-Review-Checklist.pdf
[Accessed 01 October 2018].
CRITICAL APPRAISAL SKILLS PROGRAMME. 2018b. CASP Systematic Review Checklist [Online]. Available: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Systematic-Review-Checklist.pdf
[Accessed 01 October 2018].
FEHLINGS, et al. 2017. A Clinical Practice Guideline for the Management of Patients WithAcute Spinal Cord Injury: Recommendations on the Type and Timing ofRehabilitation. Global Spine Journal,
7, 231S-238S.
FOSTER, N., BARLAS, P., CHESTERTON, L. & WONG, J. 2001.
Critically Appraised Topics (CATs). Physiotherapy,
87, 179-190.
MEHRHOLZ, J., KUGLER, J. & POHL, M. 2012. Locomotor training forwalking after spinal cord injury. Cochrane
Database Syst Rev, 11, Cd006676.
PANISSET, M. G., GALEA, M. P. & EL-ANSARY, D. 2016. Does earlyexercise attenuate muscle atrophy or bone loss after spinal cord injury? Spinal Cord, 54, 84-92.
RICE, L. A., SMITH, I., KELLEHER, A. R., GREENWALD, K., HOELMER, C.
& BONINGER, M. L. 2013. Impact of the clinical practice guideline forpreservation of upper limb function on transfer skills of persons with acutespinal cord injury. Arch Phys Med Rehabil,
94, 1230-46.
TSE, C. M., CHISHOLM, A. E., LAM, T. & ENG, J. J. 2018. Asystematic review of the effectiveness of task-specific rehabilitationinterventions for improving independent sitting and standing function in spinalcord injury. J Spinal Cord Med, 41, 254-266.
WESSELS, M., LUCAS, C., ERIKS, I. & DE GROOT, S. 2010. Bodyweight-supported gait training for restoration of walking in people with anincomplete spinal cord injury: a systematic review. J Rehabil Med, 42,
513-9.
No comments:
Post a Comment